Ashman Phenomenon: A Deep Dive into Its Mechanism and Physiology
Jan 03, 2025Ashman phenomenon is a fascinating electrocardiographic finding characterized by an aberrantly conducted supraventricular beat. Often seen in atrial fibrillation (AF) or with premature atrial contractions (PACs), it is caused by the rate-dependent refractory properties of the bundle branches. Understanding this phenomenon requires a detailed look at the physiology of the cardiac action potential and the behavior of the conduction system during variable heart rates.
This post explores the mechanism of Ashman phenomenon in the context of atrial fibrillation and premature atrial contractions, with special attention to the differing action potential durations of the right and left bundle branches.
The Electrophysiologic Basis of Ashman Phenomenon
Ashman phenomenon occurs due to an interplay between cycle length-dependent refractoriness and the differential recovery times of the right and left bundle branches. These factors lead to aberrant conduction during specific conditions. Let’s break this down step by step.
1. The Role of Refractoriness
The refractory period of cardiac tissue, including the bundle branches, is dependent on the preceding cycle length**:
- Short cycle lengths (faster heart rates): Shorter refractory periods.
- Long cycle lengths (slower heart rates): Longer refractory periods.
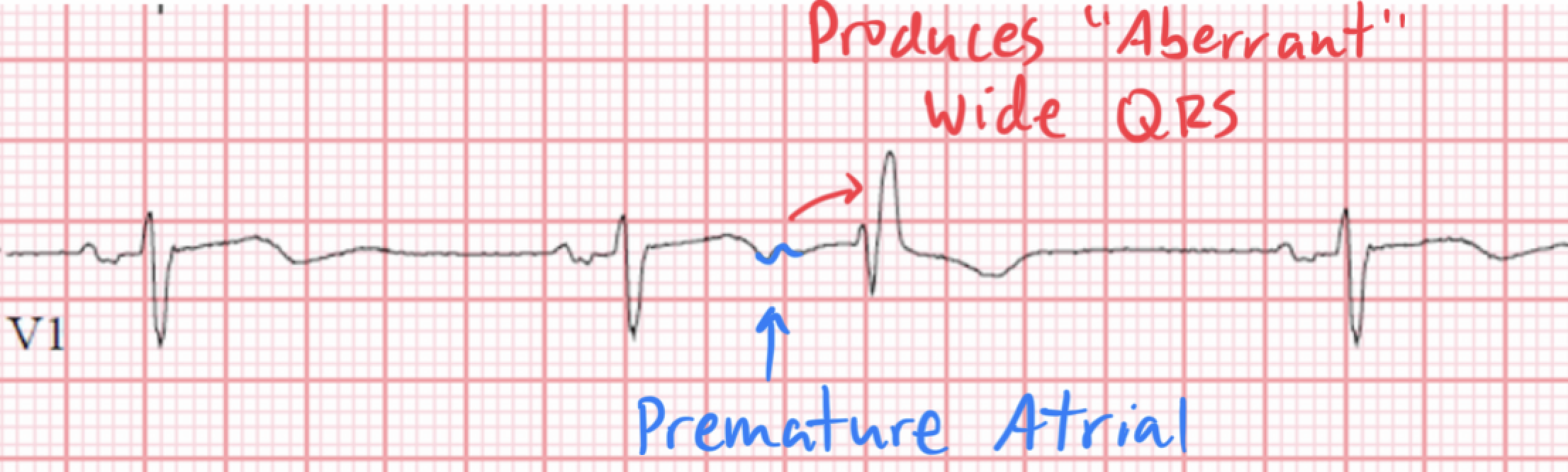
When a shorter cycle (e.g., a PAC or an irregularly timed beat in AF) follows a longer cycle, the conduction system may still be partially refractory. If the impulse encounters tissue that is slow to recover (e.g., one of the bundle branches), it results in aberrant conduction, producing a wide QRS complex that mimics a bundle branch block.
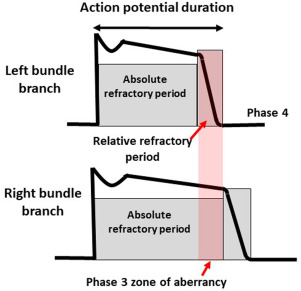
2. Action Potential Duration and Bundle Branch Recovery
The action potential duration and refractory properties of the right bundle branch (RBB) and left bundle branch (LBB) play a critical role:
- The RBB typically has a longer refractory period than the LBB.
- As a result, the RBB is more likely to remain refractory when a premature impulse occurs, leading to delayed conduction through the RBB and a right bundle branch block (RBBB) pattern on the ECG.
This differential recovery explains why Ashman phenomenon most commonly presents with an RBBB morphology.
Ashman Phenomenon in Atrial Fibrillation
Atrial fibrillation is a classic setting for Ashman phenomenon due to its hallmark irregularly irregular rhythm. The varying cycle lengths between successive R-R intervals set the stage for the phenomenon.
Mechanism in AF
1. Long-Short Sequence:
- A longer R-R interval allows the bundle branches to recover completely and reset their refractory periods.
- A shorter R-R interval (following the long interval) may result in the RBB remaining refractory due to its slower recovery time compared to the LBB.
- The next atrial impulse conducts aberrantly through the RBB, producing a wide QRS complex with an RBBB pattern.
2. Irregular Timing of Atrial Impulses:
- In AF, rapid and irregular atrial impulses bombard the AV node, leading to variable ventricular responses.
- This variability increases the likelihood of long-short R-R sequences, which favor the development of Ashman phenomenon.

Clinical Implications in AF
- The wide QRS complexes seen in Ashman phenomenon can be misinterpreted as ventricular ectopy or sustained ventricular tachycardia.
- Recognizing the RBBB morphology and its relationship to preceding cycle lengths is crucial for accurate diagnosis.
Ashman Phenomenon with Premature Atrial Contractions (PACs)
PACs are another common setting for Ashman phenomenon, though the mechanism differs slightly from that in atrial fibrillation.
Mechanism in PACs
1. Timing of the PAC:
- A PAC that occurs early, after a relatively long preceding cycle, encounters a partially refractory bundle branch (typically the RBB).
- Aberrant conduction through the RBB results in a wide QRS complex with an RBBB morphology.
2. Refractoriness and PAC Timing:
- If the PAC occurs late enough that both bundle branches have recovered, normal conduction occurs.
- The closer the PAC follows a long cycle, the higher the likelihood of aberrancy.
Clinical Implications in PACs
- Aberrantly conducted PACs can mimic ventricular ectopy, leading to potential diagnostic confusion.
- Carefully analyzing the relationship between the PAC and the preceding cycle length can help identify Ashman phenomenon.
Distinguishing Ashman Phenomenon from Ventricular Ectopy
One of the biggest challenges in clinical practice is distinguishing Ashman phenomenon from ventricular ectopy. Key features of Ashman phenomenon include:
1. Irregular Rhythm: Often occurs in the context of AF or PACs with a preceding long-short cycle.
2. QRS Morphology: Wide QRS complexes, typically with an RBBB pattern.
3. Pattern Recognition: Aberrant conduction is linked to the timing of the preceding cycles, not random as in true ventricular ectopy.
Ashman Phenomenon and the Bundle Branch Action Potential
Right Bundle Branch (RBB)
- The RBB has a longer action potential duration and refractory period compared to the LBB.
- After a long cycle, the RBB is slower to recover and more likely to conduct aberrantly when a short cycle follows.
Left Bundle Branch (LBB)
- The LBB has a shorter refractory period and is less commonly involved in Ashman phenomenon.
- Aberrant conduction through the LBB (resulting in an LBBB pattern) is rare in comparison.
Why the Difference?
The differential recovery times are influenced by intrinsic differences in ion channel kinetics and action potential properties between the RBB and LBB. This physiology underpins the characteristic RBBB morphology seen in Ashman phenomenon.
Clinical Pearls for Ashman Phenomenon
1. Context Is Key: Ashman phenomenon typically occurs in the setting of irregular rhythms like atrial fibrillation or PACs.
2. Cycle Length Matters: Look for a long-short R-R interval preceding the aberrant QRS complex.
3. Morphology Clues: The RBBB pattern of the wide QRS complex can help distinguish Ashman phenomenon from other causes of wide-complex rhythms.
4. Avoid Misdiagnosis: Misinterpreting Ashman phenomenon as ventricular ectopy or ventricular tachycardia can lead to inappropriate management.
Hope this helps!
-Reid
ECG Lectures with Reid